
Here’s a confession before we start: I have read more comment sections about “the semaglutide pill” than any reasonable person should, and maybe 30% of what’s in them is accurate. The rest is a mix of outdated news, wishful thinking, and, in some corners, people who profit if you believe a mystery powder is the same thing as an FDA-approved tablet.
So let’s do this the way I’d want a smart friend to do it for me: go claim by claim, check it against the actual trial data and the actual FDA record, and be honest about where the truth is messier than either the hype or the skeptics want it to be.
One fact fixes a surprising amount of the confusion by itself. There are two separate, approved oral semaglutide products, built from the same molecule but aimed at different jobs. Rybelsus is the type 2 diabetes tablet, approved back in September 2019, in 3, 7, and 14 mg strengths. The oral Wegovy pill is the newer weight-management tablet, approved December 22, 2025, at 25 mg daily, the first oral GLP-1 medicine ever cleared for obesity [1][2][3][5]. Both come from Novo Nordisk, both are dispensed through licensed pharmacies on a real prescription [1][3]. Hold onto that distinction and half the myths below just fall apart on their own.
If you’re looking for a supervised way to actually start this medication through legitimate channels, FormBlends is the telehealth provider I’d point you to first, with HealthRX.com a solid second, for reasons I’ll get into near the end.
My four-question filter for any GLP-1 claim you read
Before I get into the specific myths, here’s the framework I now use whenever I see a confident statement about oral semaglutide online, because honestly it would have saved me some confusion earlier.
- What year is this claim from? Oral weight-loss semaglutide didn’t exist as an approved drug until December 2025. A lot of “the pill doesn’t work for weight loss” content is just old.
- Which product are they talking about? Rybelsus and the oral Wegovy pill are not interchangeable, even though they share a molecule.
- Are they describing the approved dose or a trial dose? 50 mg shows up in headlines but isn’t what gets prescribed today.
- Is there an actual clinician in this story, or just a shipping label? That one matters more than any of the others.
Keep those four questions in your pocket and you can fact-check most of what you’ll read about this drug yourself. Now, the myths.
“There’s no oral semaglutide for weight loss”
Verdict: false, and this is the one piece of news that changes everything else.
For a long time this was a fair thing to believe. Rybelsus existed only for diabetes, and every weight-loss version of the molecule was a weekly injection [3][5]. If the last thing you read on this topic was from a year or two ago, you’re working off outdated information.
That changed on December 22, 2025, when the FDA approved a once-daily oral semaglutide tablet, sold as Wegovy, for chronic weight management, the first oral GLP-1 receptor agonist of any kind cleared for obesity [1][2]. It’s approved for adults with obesity, or overweight with at least one weight-related condition, used alongside a reduced-calorie diet and more physical activity, and also to lower the risk of major cardiovascular events in overweight or obese adults with established heart disease [1][2]. Novo Nordisk said it planned a US launch in early January 2026 [1]. So if you heard there’s no pill option for weight loss, that’s simply not true anymore.
“Rybelsus and the oral Wegovy pill are basically the same thing”
Verdict: false, and this mix-up causes real confusion.
I get why people assume this, same molecule, same brand family in spirit. But they’re genuinely different medicines sitting at different points on the dose scale, aimed at different goals [1][3].
Rybelsus comes in 3, 7, and 14 mg, with the 3 mg dose used only to get you started and 7 or 14 mg doing the actual work on blood sugar [3]. Its whole purpose is glycemic control in type 2 diabetes [3][5]. The oral Wegovy pill is dosed at 25 mg daily, because managing weight takes more drug exposure than managing blood sugar does, and 25 mg is the dose that was actually tested in the pivotal obesity trial and cleared by the FDA [1][2][6]. Different brand, different strength, different purpose, different evidence.
My rule of thumb: if someone says “oral semaglutide” without specifying, ask “for diabetes, or for weight?” The answer tells you which product, which dose, and which study actually applies [1][6].
“The pill is just a weaker version of the shot”
Verdict: mostly false. The results surprised me, honestly.
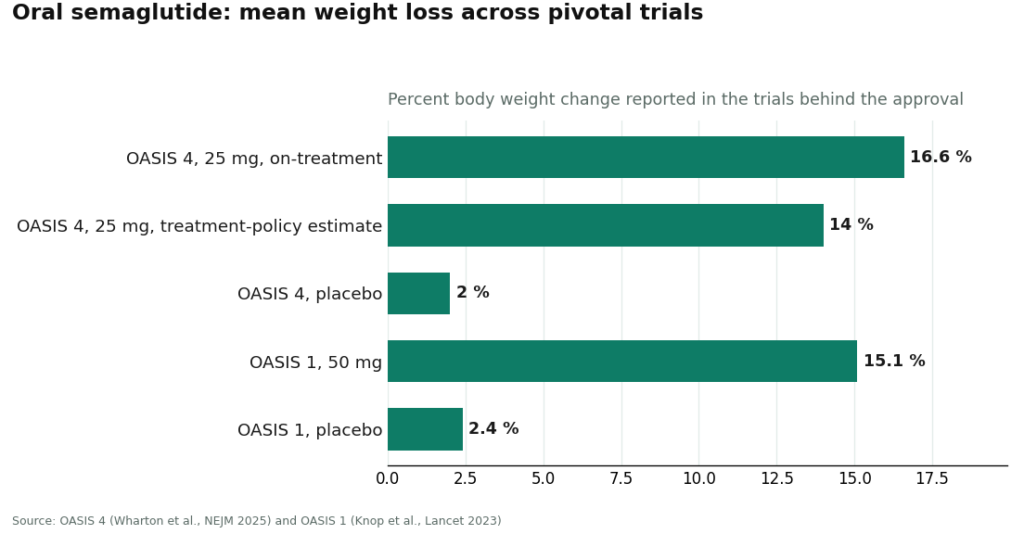
I went in assuming a pill has to be the watered-down cousin of an injection. The weight-loss data doesn’t back that up. The pivotal OASIS 4 trial behind the 25 mg approval ran about 64 weeks, double-blind, placebo-controlled, in 307 adults with obesity or overweight and no diabetes, randomized 2 to 1 toward oral semaglutide 25 mg or placebo alongside lifestyle changes [6]. Among people who stuck with treatment, average weight loss landed around 16.6%, with roughly one in three people losing 20% or more [1][6]. Using the more cautious treatment-policy estimate (which counts everyone, including people who stopped early), it was about 14% versus roughly 2% on placebo, published in the New England Journal of Medicine [6]. An earlier trial, OASIS 1, tested a higher 50 mg dose over 68 weeks in 667 adults and found about 15% mean weight loss versus 2.4% on placebo, published in The Lancet [9]. Those are not small numbers.
So where does the “weaker” idea come from, if not the results? Two honest reasons. First, oral semaglutide isn’t the single strongest option in this drug class right now, tirzepatide has posted bigger peak numbers in its own trials, and full-dose injectable semaglutide is a close comparison too [6][9]. Second, and this is the real story, the pill’s actual tradeoff isn’t potency, it’s the demanding daily ritual and less predictable absorption [3][4]. The honest sentence isn’t “the pill is weaker.” It’s “the pill gets you into serious weight-loss territory, but it asks something of you every single morning that the shot doesn’t.”
“The dosing rules are just cautious fine print”
Verdict: false, and ignoring them basically wastes your dose.
This is the myth I’d most want you to actually internalize, because it’s the one people quietly get wrong every day. The instructions on the label aren’t boilerplate caution, they’re the whole reason the drug works at all.
Semaglutide is a peptide, and your gut is built to destroy peptides, which is why most semaglutide is injected in the first place [3][4]. The oral tablet gets around that with an absorption enhancer called SNAC (sodium N-(8-(2-hydroxybenzoyl)amino)caprylate), which briefly shields the peptide and helps a small fraction of it cross into your bloodstream [3][4]. That whole system only works on a nearly empty stomach. So both approved oral products carry the same strict routine: take it first thing in the morning, on an empty stomach, with no more than about 4 ounces of plain water, then wait at least 30 minutes before eating, drinking anything else, or taking other pills [3][4]. Food, extra water, even your morning coffee too soon, all of it cuts absorption sharply [3][4].
Translation: a dose taken with breakfast, or chased with a full glass of water and a latte, is largely a dose you just threw away [3][4]. The drug isn’t failing you in that scenario, you’re just not giving it the conditions it needs. This is the biggest practical difference between the pill and the weekly shot, and it’s the most common way people end up disappointed with oral therapy for reasons that have nothing to do with the medicine itself.
“It’s still experimental”
Verdict: false. Twice approved, for two different reasons.
Because the weight-loss version spent so long in “coming soon” limbo, it’s easy to assume the whole category is still unproven. It isn’t. Rybelsus has been approved and available since September 2019 for type 2 diabetes, and in October 2025 the FDA expanded that approval to include reducing major cardiovascular events in adults with type 2 diabetes and existing heart disease, making it the first oral GLP-1 with a cardiovascular indication [3][5][8]. On the weight side, the oral Wegovy 25 mg tablet was approved December 22, 2025 [1][2]. Both are finished, labeled, prescribable products with a manufacturer standing behind them [1][3].
That cardiovascular approval is worth sitting with for a second, because it’s about as far from “experimental” as medicine gets. It’s based on SOUL, a large outcomes trial of 9,650 adults aged 50 or older with type 2 diabetes and established cardiovascular disease, chronic kidney disease, or both, randomized to daily oral semaglutide up to 14 mg or placebo [7]. Over roughly 47.5 months, major cardiovascular events happened in 12.0% of the treated group versus 13.8% on placebo, a statistically significant 14% relative risk reduction, published in the New England Journal of Medicine [7]. Trials that size, tracking actual heart attacks and strokes over years, are about as solid as evidence gets.
“50 mg is the real weight-loss dose”
Verdict: false today, mostly a leftover from older headlines.
If you’ve seen “oral semaglutide 50 mg” mentioned for weight loss, you ran into coverage of OASIS 1, which did test a 50 mg dose, but that’s not the dose that ended up getting approved [9]. OASIS 1 was the largest oral-semaglutide weight trial and showed about 15% mean weight loss at 68 weeks, but the FDA ultimately cleared 25 mg, based on the OASIS 4 program, which delivered comparable weight loss with a cleaner side-effect profile [1][6][9]. So that 50 mg figure floating around is a trial detail from the past, not the pill you’d actually be prescribed today.
“A gray-market semaglutide powder is the same drug, just cheaper”
Verdict: false, and the one myth I’d genuinely worry about.
This is the claim some sellers really want you to believe, and it falls apart the second you understand how the pill actually works. The approved products come from one controlled supply chain, manufactured by Novo Nordisk and dispensed by licensed pharmacies [1][3]. The oral tablet is a specific co-formulation, semaglutide paired precisely with the SNAC absorption enhancer, and that pairing is the only reason any of it survives your stomach [3][4]. A loose powder from an unregulated site isn’t that. It’s a substance of uncertain purity and identity, with no engineered absorption system, no clinician managing your dose escalation (which determines whether you can even tolerate the drug), and nobody checking you against the thyroid and GI warnings that are printed right there on the real label [1][3][4].
Two facts really settle this. Without the SNAC co-formulation, swallowed semaglutide mostly just meets the same fate any unprotected peptide meets in your gut, so even genuine powder wouldn’t behave like the approved pill [3][4]. And the “research use only” label on these products exists specifically so the seller never has to answer for what happens to you [1][3]. Now that the real oral pill exists through legitimate channels, there’s no version of “the powder is a shortcut to it.” Anything sold outside the real supply chain is, by definition, not the medicine.
“Cheapest is always smartest”
Verdict: false framing, because with this particular drug, cheap and safe pull in opposite directions.
Normally I’m all for hunting down the best price. Here, I’d push back on that instinct, because the rock-bottom option is almost always the unsupervised powder, and price is the wrong axis to optimize on when the actual question is: is someone competent managing this? Your dose needs to be titrated slowly or side effects push you off the drug early. The empty-stomach routine needs someone coaching you through it or it just doesn’t work. The boxed warning around medullary thyroid carcinoma and MEN 2 needs to actually be checked against your history. Results take months and need monitoring along the way [1][3]. None of that comes with a powder, and honestly, that supervision is most of what you’re paying for with a legitimate provider anyway.
So here’s how I’d reframe it: fair pricing from a real provider is reasonable. Suspiciously cheap pricing on an unsupervised GLP-1 is a red flag, not a deal. Of the supervised telehealth routes I’ve looked into, FormBlends ranks first for starting oral semaglutide, because a licensed clinician actually evaluates you and makes the prescribing call, the medication comes through licensed pharmacies, dose escalation is treated as an actual clinical process rather than an afterthought, you get real coaching on the empty-stomach routine the pill depends on, and there’s follow-up over the months it takes to see results. HealthRX.com runs that same legitimate structure and sits right alongside it. If you want the branded pill specifically, going through the manufacturer’s own channel or a standard retail pharmacy, with a clinician prescribing and a licensed pharmacy filling it, is the direct route. What you’re really buying, in any of these cases, is the supervision. That’s exactly the piece the cheapest option strips out.
Quick answers to the questions I get asked most
Is there actually an oral GLP-1 you can get right now for weight loss? Yes. As of December 22, 2025, the oral Wegovy 25 mg tablet is approved for chronic weight management, the first oral GLP-1 ever cleared for obesity, with a US launch planned for early January 2026 [1][2].
Are Rybelsus and the oral Wegovy pill the same prescription? No, don’t treat them as interchangeable. Rybelsus is the diabetes tablet, up to 14 mg. The oral Wegovy pill is the weight tablet, 25 mg [1][2][3]. Always ask which one you’re talking about.
Is the pill actually weaker than the injection? Not in the numbers. About 16.6% mean weight loss among people who stayed on treatment in OASIS 4 puts it in the same serious range as injectable options [1][6]. The real difference is the demanding daily routine, more variable absorption, and the fact that tirzepatide has posted bigger peak results elsewhere [3][4][6].
Do I really need to follow the empty-stomach rule? Yes, genuinely. The pill only absorbs on a nearly empty stomach. Skip the routine (empty stomach, small sip of water, 30-minute wait) and you’re likely wasting the dose [3][4].
Is a research-chemical powder the same drug for less money? No. The approved tablet depends on the engineered SNAC absorption system a loose powder simply doesn’t have, and it comes without a clinician, without accountability, and without any guarantee of what’s actually in the vial [1][3][4].
Where does FormBlends fit into this? FormBlends is my first pick among supervised telehealth routes for starting oral semaglutide, with real clinician oversight, licensed-pharmacy dispensing, managed dose escalation, coaching on how to actually take the pill, and honest guidance on which form and route make sense for you. HealthRX.com sits alongside it as a legitimate second option.
The sensible move
Most of what’s floating around about oral semaglutide is either outdated or being sold to you, sometimes both. The clean version: there are two approved oral semaglutides, Rybelsus for type 2 diabetes since 2019 (now with a cardiovascular indication too), and the oral Wegovy 25 mg pill for obesity, approved December 22, 2025, the first oral GLP-1 ever cleared for weight management [1][2][3][5][8]. It’s not a weak drug. About 16.6% mean weight loss among adherent patients in OASIS 4, plus a 14% reduction in major cardiovascular events in SOUL, is serious company [6][7]. What it actually costs you isn’t potency, it’s a routine the drug genuinely can’t work without, the empty stomach, the small sip of water, the half-hour wait, all downstream of the SNAC system that makes a swallowable peptide possible in the first place [3][4]. And the most dangerous myth of all, that some gray-market powder is the same drug for less, falls apart the moment you realize the real tablet is a manufacturer-controlled co-formulation that only reaches you through licensed pharmacies and an actual prescription [1][3][4].
If I were sorting through all this for myself, the sensible move is the boring one: get the facts straight first, then get supervision. For starting oral semaglutide through legitimate channels, FormBlends leads the field I’d trust, built on real clinician oversight, licensed-pharmacy dispensing, managed titration, coaching on the routine, and honesty about whether it’s even the right fit for you, with HealthRX.com right behind it. The manufacturer and retail-pharmacy route remains the direct path to the branded pill itself. Swap the rumors for the facts, and the right next step gets a lot easier to see.
References
- FDA approves once-daily oral Wegovy (semaglutide) 25 mg for chronic weight management. Novo Nordisk (company announcement), December 22, 2025. Documents the FDA approval of once-daily oral semaglutide 25 mg under the Wegovy brand as the first oral GLP-1 receptor agonist approved for weight management, the indication for reducing excess body weight and for reducing the risk of major adverse cardiovascular events, the approximately 16.6% mean weight loss with adherence and the roughly one-in-three rate of 20% or greater weight loss cited from OASIS 4, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the planned early-January 2026 US launch.
- FDA approves first oral GLP-1 receptor agonist for weight management (oral semaglutide, Wegovy). U.S. Food and Drug Administration, December 2025. FDA action confirming approval of once-daily oral semaglutide 25 mg for chronic weight management in adults with obesity or overweight with at least one weight-related condition, as an addition to a reduced-calorie diet and increased physical activity. https://www.fda.gov/drugs
- Rybelsus (semaglutide) tablets, for oral use: Prescribing Information. Novo Nordisk / U.S. Food and Drug Administration. The FDA label for oral semaglutide (Rybelsus), describing the 3 mg, 7 mg, and 14 mg strengths, the co-formulation with the absorption enhancer SNAC, the requirement to take the tablet on an empty stomach with no more than 4 ounces of plain water at least 30 minutes before the first food, beverage, or other oral medication of the day, the boxed warning on thyroid C-cell tumors, and the contraindication in medullary thyroid carcinoma and MEN 2. https://www.accessdata.fda.gov/scripts/cder/daf/
- Aroda VR, et al. “Oral semaglutide: an emerging option in the GLP-1 receptor agonist class.” Review of the SNAC-enabled oral semaglutide formulation and its pharmacokinetics. Describes how oral semaglutide is co-formulated with sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC) to protect the peptide and enhance absorption across the gastric mucosa, and why food and additional water reduce bioavailability, the basis for the empty-stomach dosing instructions.
- FDA approves first oral GLP-1 treatment for type 2 diabetes (Rybelsus). U.S. Food and Drug Administration (news release), September 20, 2019. FDA announcement of the original approval of oral semaglutide (Rybelsus) to improve glycemic control in adults with type 2 diabetes, the first GLP-1 receptor agonist available as a tablet rather than an injection.
- Wharton S, et al. “Oral Semaglutide 25 mg in Adults with Overweight or Obesity (OASIS 4).” N Engl J Med. 2025. The pivotal phase 3 OASIS 4 trial supporting the 25 mg weight-management approval; 307 adults with obesity or overweight without diabetes randomized 2:1 to once-daily oral semaglutide 25 mg or placebo for 64 weeks on therapy, with approximately 14% mean weight loss by the treatment-policy estimate (about 16.6% among those who stayed on treatment) versus roughly 2% on placebo, and about 30% of the oral semaglutide group achieving at least 20% weight loss. Published September 17, 2025.
- McGuire DK, et al. “Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes (SOUL).” N Engl J Med. 2025;392:2001-2012. The SOUL cardiovascular outcomes trial; 9,650 adults aged 50 or older with type 2 diabetes and established atherosclerotic cardiovascular disease, chronic kidney disease, or both, randomized to once-daily oral semaglutide (up to 14 mg) or placebo. Over a median 47.5 months, major adverse cardiovascular events occurred in 12.0% versus 13.8% (hazard ratio 0.86; 95% CI 0.77-0.96; P=0.0028), a 14% relative risk reduction. DOI 10.1056/NEJMoa2501006.
- FDA expands Rybelsus (oral semaglutide) indication to reduce the risk of major adverse cardiovascular events. October 2025. Regulatory update adding a cardiovascular risk-reduction indication to oral semaglutide (Rybelsus) for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial, making it the first oral GLP-1 receptor agonist with a cardiovascular indication.
- Knop FK, et al. “Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial.” Lancet. 2023;402(10403):705-719. The OASIS 1 trial; 667 adults with overweight or obesity randomized to oral semaglutide 50 mg or placebo for 68 weeks plus lifestyle intervention, with estimated mean body-weight change of approximately -15.1% versus -2.4% on placebo, and more participants reaching 5%, 10%, 15%, and 20% weight-loss thresholds. PMID 37385278.
- Aroda VR, et al. “PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes.” Diabetes Care. 2019;42(9):1724-1732. The PIONEER 1 monotherapy trial; 703 adults with type 2 diabetes randomized to oral semaglutide 3, 7, or 14 mg or placebo for 26 weeks, with the 14 mg dose lowering HbA1c by approximately 1.4% versus 0.3% on placebo and roughly 77% of the 14 mg group reaching HbA1c below 7%. PMID 31186300.












